Physiotherapy in Toronto for Pediatric Issues
Welcome to In Balance Physiotherapy’s Guide to Perthes Disease of the Hip.
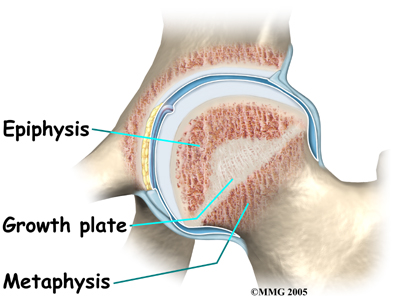
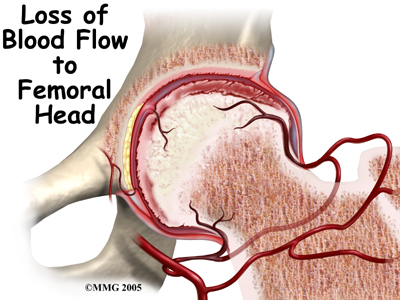
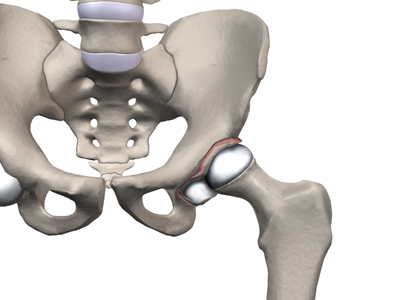
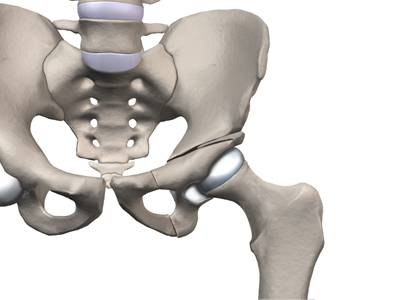
 Perthes disease is a condition that affects the hip in children between the ages of four and eight. The condition is also referred to as Legg-Calve-Perthes disease in honor of the three physicians who each separately described the disease. In this condition, the blood supply to the growth center of the hip (the capital femoral epiphysis) is disturbed, causing the bone in this area to die. The blood supply eventually returns, and the bone heals. How the bone heals determines what problems the condition will cause in later life. Perthes disease may affect both hips. In fact, 10 to 12 percent of the time the condition is bilateral (meaning that it affects both hips). This condition can lead to serious problems in the hip joint later in life.
Perthes disease is a condition that affects the hip in children between the ages of four and eight. The condition is also referred to as Legg-Calve-Perthes disease in honor of the three physicians who each separately described the disease. In this condition, the blood supply to the growth center of the hip (the capital femoral epiphysis) is disturbed, causing the bone in this area to die. The blood supply eventually returns, and the bone heals. How the bone heals determines what problems the condition will cause in later life. Perthes disease may affect both hips. In fact, 10 to 12 percent of the time the condition is bilateral (meaning that it affects both hips). This condition can lead to serious problems in the hip joint later in life.
This guide will help you understand:
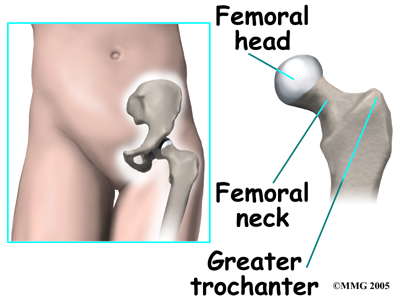
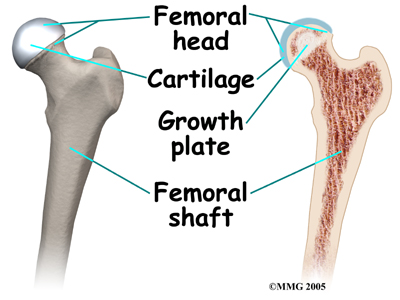
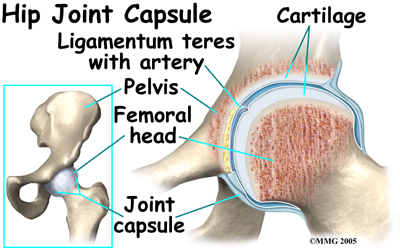
- what part of the hip is involved
- what causes the condition
- what treatment options are available
- what In Balance Physiotherapy’s approach to rehabilitation is
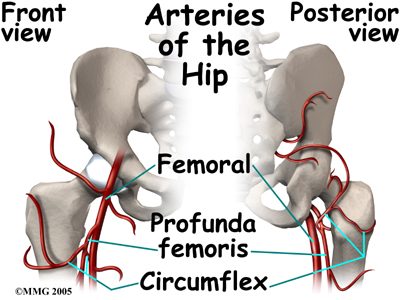
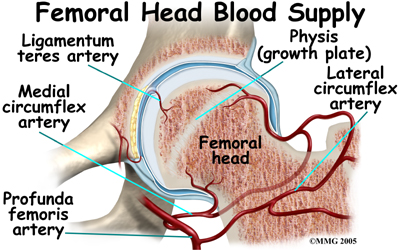
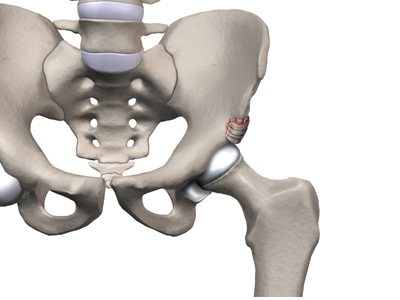
 Children who have abnormal blood clotting (a condition called thrombophilia) may also have a higher risk of developing Perthes disease. These children have blood that clots easier and quicker than normal. This may lead to blood clotting that blocks the small arteries going to the femoral head. As a result of new evidence, the certainty of thrombophilia as a cause of Perthes is now under debate. This will remain an area of study until scientists clear up the significance of thrombophilia as a possible cause of Perthes.
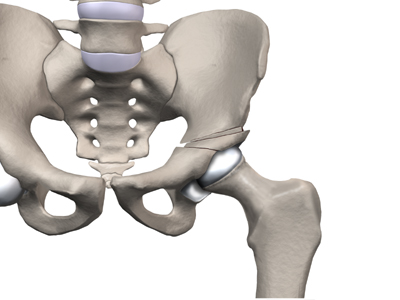
Children who have abnormal blood clotting (a condition called thrombophilia) may also have a higher risk of developing Perthes disease. These children have blood that clots easier and quicker than normal. This may lead to blood clotting that blocks the small arteries going to the femoral head. As a result of new evidence, the certainty of thrombophilia as a cause of Perthes is now under debate. This will remain an area of study until scientists clear up the significance of thrombophilia as a possible cause of Perthes.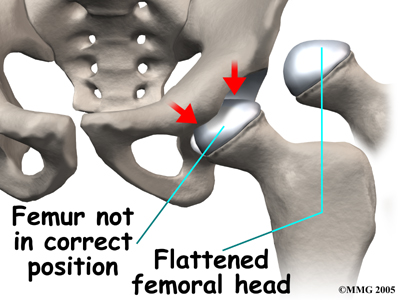 The main problem with Perthes disease is that it changes the structure of the hip joint. How much it affects the way the hip joint works depends on how much the hip joint is deformed. Muscle weakness and atrophy affecting the thigh and calf muscles may develop over time. The affected leg can shorten as a result of the changes in the hip. The result may be a significant leg length difference. Problems later in life are more likely the greater the deformity after the condition has healed.
The main problem with Perthes disease is that it changes the structure of the hip joint. How much it affects the way the hip joint works depends on how much the hip joint is deformed. Muscle weakness and atrophy affecting the thigh and calf muscles may develop over time. The affected leg can shorten as a result of the changes in the hip. The result may be a significant leg length difference. Problems later in life are more likely the greater the deformity after the condition has healed.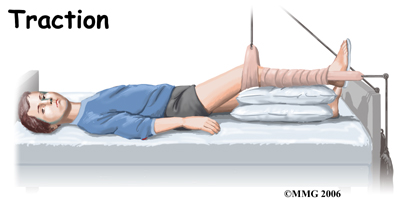
 Physiotherapy while in the hospital is used to restore the hip motion as the inflammation comes under control. A physiotherapist will visit your child in their room and assist them with some gentle hip rotation and abduction exercises (taking the leg out to the side.) These exercises will maintain and improve range of motion but will also assist in moving the fluid inside the hip joint, which assists with joint nutrition and is crucial to healing. They will also show you and your child how to continue the exercises independently once your child leaves the hospital if you will be using a home traction unit, and may prescribe further simple exercises that your child should do once they are no longer in traction. Your physiotherapist may even recommend that your child do some exercises in the pool to take advantage of the hydrostatic properties of the water to gain range of motion with less weight bearing impact.
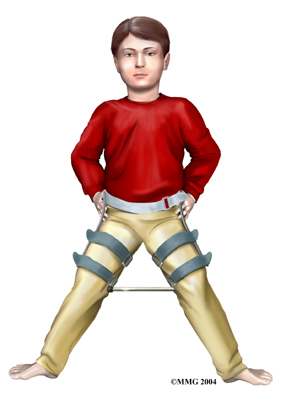
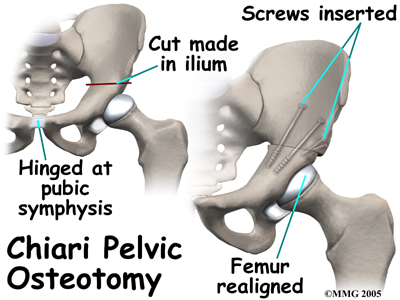
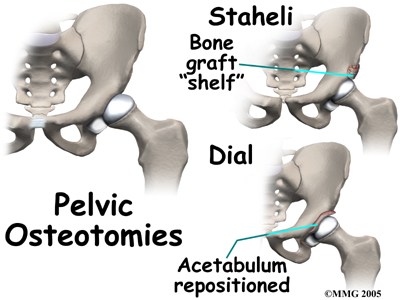
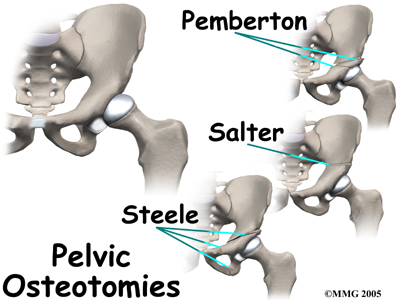
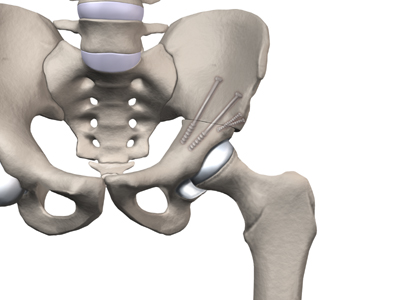
Physiotherapy while in the hospital is used to restore the hip motion as the inflammation comes under control. A physiotherapist will visit your child in their room and assist them with some gentle hip rotation and abduction exercises (taking the leg out to the side.) These exercises will maintain and improve range of motion but will also assist in moving the fluid inside the hip joint, which assists with joint nutrition and is crucial to healing. They will also show you and your child how to continue the exercises independently once your child leaves the hospital if you will be using a home traction unit, and may prescribe further simple exercises that your child should do once they are no longer in traction. Your physiotherapist may even recommend that your child do some exercises in the pool to take advantage of the hydrostatic properties of the water to gain range of motion with less weight bearing impact. Surgical treatment for containment may be best in older children who are not compliant with brace treatment or where the psychological effects of wearing braces may outweigh the benefits. Surgical containment does not require long-term braces or casts. Once the procedure has been performed and the bones have healed, the child can pursue normal activities as tolerated.
Surgical treatment for containment may be best in older children who are not compliant with brace treatment or where the psychological effects of wearing braces may outweigh the benefits. Surgical containment does not require long-term braces or casts. Once the procedure has been performed and the bones have healed, the child can pursue normal activities as tolerated.


Discussion (0)
There are no comments for this doc yet.
Comment posting has been disabled on this doc.